If you use imagery rescripting in your Schema Therapy practice, you’ve likely heard a client say something like:
“But that didn’t really happen. That’s not real.”
It’s a powerful moment—one that can derail the session or open the door to meaningful emotional healing, depending on how we respond.
In this blog, we’ll walk through a step-by-step framework you can use to respond compassionately and effectively when clients push back on the emotional reality of imagery work. You’ll also find sample language, an optional metaphor, and a full therapist transcript to help you ground this in your own voice.
Download the Free Resource here.
Why Clients Resist Imagery
Clients often come out of a rescripting experience with deep emotions—and sometimes, deep confusion. They may intellectually understand the exercise, but emotionally, it can feel jarring:
- “It’s not what happened.”
- “You weren’t there.”
- “That’s a lie.”
These responses aren’t wrong. They’re protective. And they’re invitations to slow down and help the client integrate what just happened.
A Step-by-Step Framework to Respond
1. Validate the Client’s Reality
Start by acknowledging the truth in their observation.
“You’re right. That didn’t happen in real life. It’s completely valid to say that.”
2. Acknowledge the Limits of Therapy
Be honest and clear: therapy doesn’t rewrite history.
“Nothing we do here can change what actually happened to you.”
3. Reframe the Aim of Imagery Rescripting
Shift the focus from facts to emotional repair.
“The goal isn’t to change the past. It’s to help that younger part of you feel safe, seen, and less alone—now.”
4. Link Present-Day Struggles to the Past
Use mode language to connect their present distress to unresolved childhood trauma.
“Even now, little Jenny still feels scared when she’s on a train or in a crowd.”
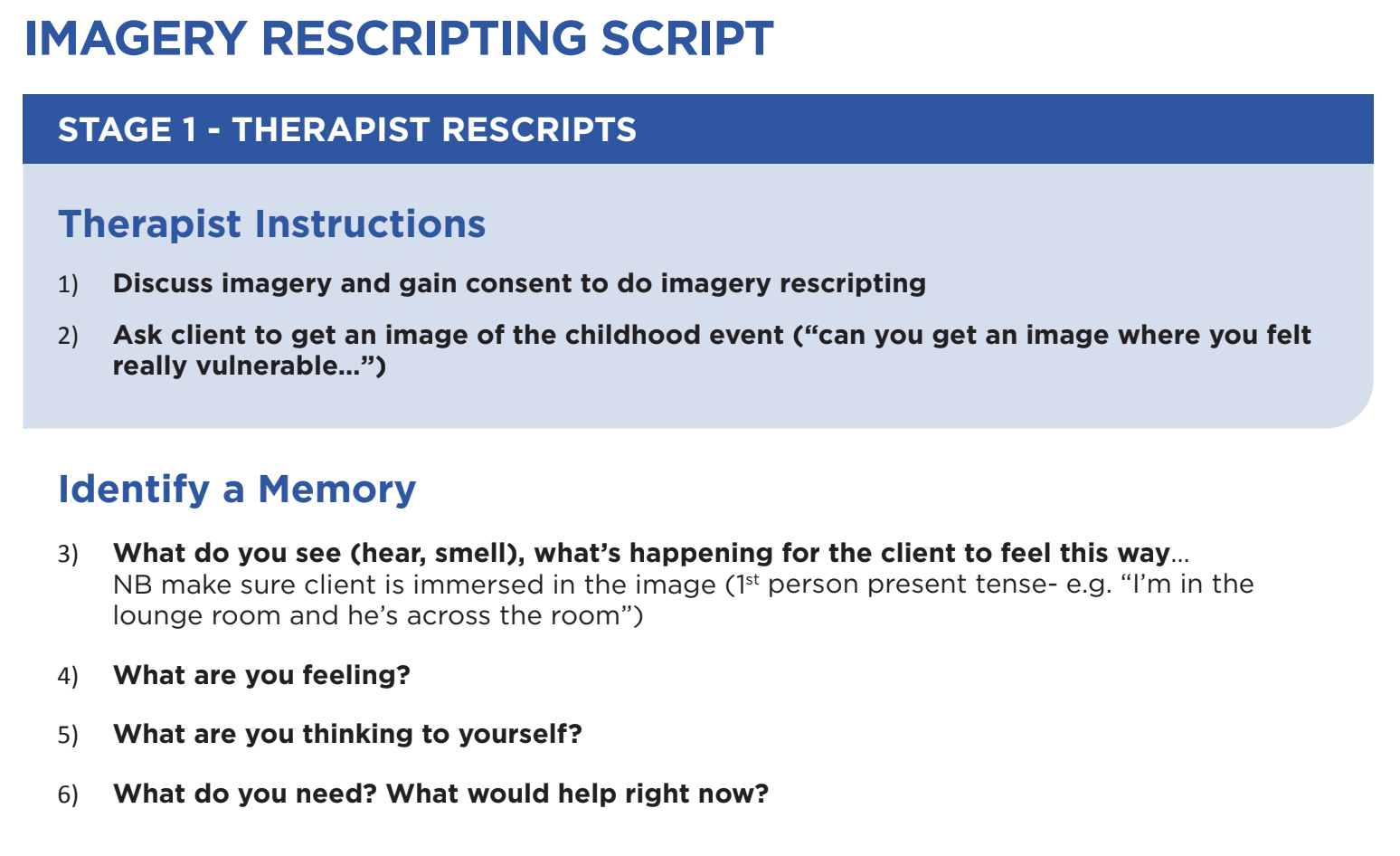
5. Justify the Use of Imagery
Normalize imagination as a therapeutic tool.
“We’re using imagery to give that younger part something she never got: protection, care, validation.”
6. Emphasize Emotional Learning
Help the client understand that while history can’t change, emotional responses can.
“We’re not rewriting facts—we’re changing how those memories feel.”
7. Invite Reflection and Integration
Ask what part of the experience (if any) felt soothing or meaningful.
“Did any part of you feel even a little comforted during that?”
8. If Resistance Continues – Look for a Coping Mode
Persistent resistance may indicate a blocking mode at play. You’ll need to engage with that mode before continuing with imagery work.
Optional Metaphor: The Broccoli Analogy
Some clients benefit from metaphor to make sense of emotional dissonance:
“It’s like trying broccoli for the first time when you’re used to eating chips. It feels weird—but it might be what your body actually needs.”
Sample Therapist Language
Here’s a full sample response you might adapt in-session:
“Okay, Jenny… I think I need to apologize. When you say, ‘That’s not real,’ I wonder if I haven’t explained this well enough. Because you’re absolutely right—what we did in imagery didn’t happen in real life. Nothing we do here can change that history, and I want to honour what you went through.”
“This exercise isn’t about pretending it didn’t happen or rewriting your story. It’s about helping little Jenny—the part of you still carrying the fear and pain—realize she’s no longer alone. We can’t change the facts, but we can work on how those facts live in your body. That’s what we’re doing here.”
“We’re helping her feel seen. Safe. Protected. And that’s what starts to shift how these memories affect you today.”
Free Resource Download: Imagery Rescripting
Imagery rescripting can be one of the most healing interventions in Schema Therapy—but only if clients feel safe and understood throughout the process.
When a client says, “But that wasn’t real,” it’s not a failure. It’s a moment of truth. With the right response, it can be the very turning point that helps them take the work deeper.
Download the free resource.
We hope this framework supports you in navigating those moments with confidence, compassion, and clinical clarity.
—
Want more tools like this?
Explore our full training library at SchemaTherapyTrainingOnline.com.
—
© Chris Hayes & Rob Brockman, 2024
You’re welcome to share this article with colleagues—please credit the original source.